If you run a medical practice, delayed payments and claim denials from coding errors can disrupt cash flow, stress your team, and pull focus from patient care. Studies show up to 20% of claims are initially denied due to coding issues, with small mistakes like mismatched diagnosis codes adding weeks—or months—to reimbursements.
These errors don’t just hit revenue; they trigger compliance headaches and audits that busy providers can’t afford. Even a single incorrect code can flag medical necessity, leading to rejected claims or underpayments that compound over high patient volumes.
Understanding medical coding empowers you to oversee documentation, spot trends in denials, and protect your practice’s bottom line—without needing to code yourself. To understand why this happens, let’s first define what medical coding actually is.
What is Medical Coding?
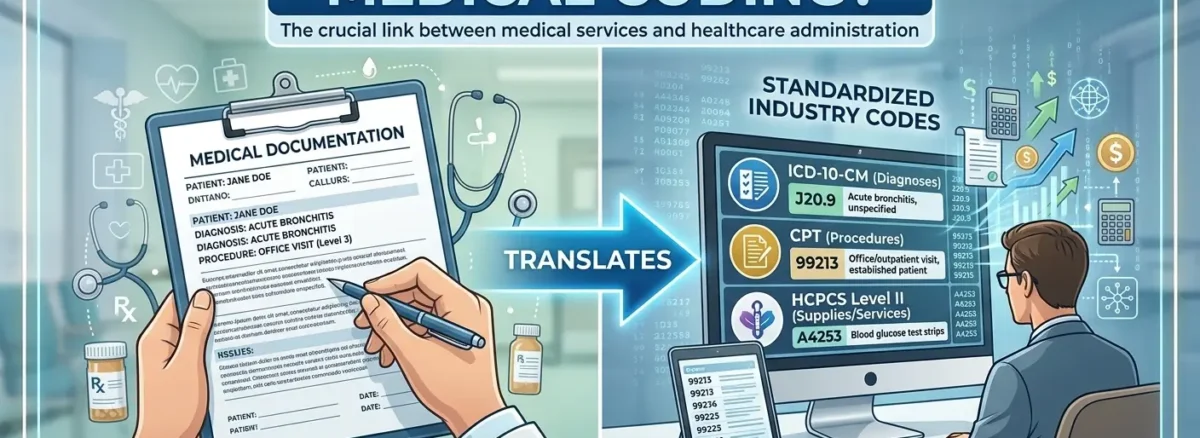
Medical coding converts your patient diagnoses, procedures, and services into standardized alphanumeric codes used for billing, reporting, and insurance claims.
Think of it as translating your clinical notes—a flu diagnosis or knee X-ray—into a universal language that payers like Medicare or private insurers instantly recognize. It’s not just paperwork; these codes directly determine if your practice gets paid fairly and on time.
Here’s a simple example of how it works in everyday visits:
| Patient Visit | Diagnosis | Procedure | Codes Submitted |
| Flu symptoms | Influenza | Office visit | ICD + CPT |
| Knee pain | Pain in right knee (M25.561) | X-ray | CPT code |
In the table above, ICD codes capture the “why” (like influenza or knee pain), while CPT codes cover the “what” (office visit or X-ray). This pairing ensures payers see the full picture for quick approval. Providers benefit by knowing that clear documentation leads to accurate coding and fewer payment hiccups.
The 3 Main Types of Medical Codes Providers Should Know
As a provider, you don’t need to memorize codes, but knowing these three main types helps you understand why documentation matters for approvals and payments.
A. ICD-10 Codes
ICD-10 codes identify patient diagnoses and reasons for visits, like J11.1 for influenza. They prove medical necessity, which payers require before reimbursing services—get this wrong, and claims bounce back fast.
B. CPT Codes
CPT codes, maintained by the American Medical Association, describe procedures and services you perform, such as 99213 for a standard office visit. These directly set your reimbursement rate, so precise matching to your notes keeps revenue steady.
C. HCPCS Codes
HCPCS codes cover supplies, equipment, injections, and Medicare-specific services—like E0601 for a cane. They’re essential for durable medical equipment (DME) or non-physician services, ensuring nothing falls through billing cracks.
| Code Type | Purpose | Why It Matters to Providers |
| ICD-10 | Diagnosis | Supports medical necessity |
| CPT | Services performed | Determines payment amount |
| HCPCS | Supplies/Medicare | Required for certain claims |
Mastering these basics lets you guide your team toward cleaner claims and fewer denials.
How Medical Coding Works in a Medical Practice
Medical coding fits seamlessly into your daily workflow, turning patient encounters into payable claims without extra hassle.
Here’s the simple step-by-step process:
- Provider Documents Care: You note the diagnosis (e.g., flu symptoms), procedures (e.g., exam), and services in the patient’s chart.
- Coder Reviews and Assigns Codes: A certified coder translates your notes into ICD-10, CPT, or HCPCS codes, ensuring everything matches medical necessity.
- Claim Submission: Coded claims go to payers via electronic systems like clearinghouses.
- Insurance Review: Payers check codes for accuracy—right diagnosis linked to service?—then approve or deny.
- Payment: Approved claims trigger reimbursements, typically within 14-30 days.
Oversight comes from groups like the Centers for Medicare & Medicaid Services (CMS), which set standards to protect patients and practices. This flow keeps your revenue cycle humming, but gaps in any step—like vague notes—slow it down.
Why Accurate Medical Coding Is Critical for Providers
Accurate medical coding safeguards your practice’s revenue while minimizing risks that could derail operations.
It ensures proper reimbursement by linking services to correct codes, so a routine office visit (CPT 99213) tied to flu (ICD-10 J11.1) pays what it’s worth—no shortfalls.
Claim denials drop sharply; vague or mismatched codes account for many rejections, forcing costly resubmissions and delaying cash flow by weeks.
Audit risks shrink, protecting against penalties from overcoding (billing higher than justified) or undercoding (missing billable work). The Office of Inspector General watches closely, and clean coding keeps you compliant.
Finally, it streamlines revenue cycle efficiency, improving tracking for better financial insights and faster payments. Strong coding turns potential losses into steady income, letting you focus on care.
Common Medical Coding Errors (and Their Financial Impact)
Even experienced teams make coding slips that hit your bottom line—knowing these helps you prevent them upfront.
Here’s a breakdown of frequent issues:
| Coding Error | Why It Happens | Financial Impact |
| Wrong diagnosis code | Incomplete documentation | Claim denial; resubmit delays revenue by 30+ days |
| Missing modifier | Coding oversight | Reduced payment or partial denial |
| Upcoding | Incorrect interpretation | Audit risk & penalties up to $10,000 per claim |
| Downcoding | Conservative coding | Revenue loss from underbilling services |
These errors compound quickly: a single denied claim might cost $100–$500 in lost time and follow-up, while patterns erode payer relationships and trigger reviews. For busy practices, repeated denials slow cash flow, forcing reliance on lines of credit. Catching them through clear notes and team training keeps money moving steadily.
Medical Coding vs. Medical Billing: What Providers Need to Know
Many providers mix up coding and billing, but clarifying the difference streamlines your revenue cycle and cuts confusion.
Coding happens first: it assigns precise ICD-10, CPT, and HCPCS codes to your documentation, focusing on accuracy to support medical necessity.
Billing follows: it packages those codes into claims, submits them to payers, and chases payments or appeals denials.
| Medical Coding | Medical Billing |
| Assigns codes to services | Submits claims to payers |
| Focuses on documentation accuracy | Focuses on payment collection |
| Happens first in workflow | Happens after coding is done |
Coding errors directly sabotage billing success—think denied claims from mismatched codes. When both align, your practice enjoys smoother reimbursements and healthier cash flow.
Do Providers Need to Handle Medical Coding Themselves?
You don’t need to code every chart yourself—most providers delegate to certified staff or services—but staying involved protects your revenue.
Your role stays simple yet vital:
- Document clearly: Specific notes (e.g., “right knee pain with swelling”) make coding accurate.
- Understand denial trends: Review reports to spot patterns, like frequent ICD-10 mismatches.
- Ensure medical necessity: Link diagnoses to services so payers approve without pushback.
Signs you may need extra coding support:
- High denial rates over 10-15%.
- Repeated payer rejections or corrections.
- Delayed reimbursements are slowing cash flow.
- Growing patient volume without a dedicated coder.
- No certified staff (CPC, CCS) on board.
How MedAce Helps Providers Simplify Medical Coding
MedAce takes the coding burden off your shoulders with certified specialists who ensure every claim is accurate, compliant, and positioned for fast payment.
Our team delivers:
- Expert coding: Precise ICD-10, CPT, and HCPCS assignments tailored to your documentation, slashing denial rates by up to 40%.
- Denial reduction strategies: Proactive audits catch errors early, turning potential rejections into approvals.
- Compliance focus: We align with CMS and OIG guidelines, minimizing audit risks and penalties.
- Ongoing quality checks: Regular reviews and updates keep your coding current amid yearly changes.
- Faster reimbursements: Streamlined processes cut processing times, boosting cash flow for practice growth.
Providers partnering with MedAce report steadier revenue, less administrative stress, and more time for what matters—patient care. We protect your bottom line while you focus on medicine.
Ready to simplify? Request a free coding audit or consultation today. See how we can improve your claim accuracy and get paid on time.
Frequently Asked Questions
1. What is the difference between an ICD-10 code and a CPT code?
Think of medical coding as a two-part sentence. The ICD-10 code is the “why”—it describes the patient’s diagnosis or the reason they came to see you (like a sore throat or a broken arm). The CPT code is the “what”—it describes the specific service or procedure you performed (like an office visit, a strep test, or an X-ray). To get paid, the “why” must always justify the “what.”
2. Why do insurance companies deny claims if the coding isn’t “specific” enough?
Insurance companies use a concept called “medical necessity.” If you use a vague diagnosis code (like “pain”) instead of a specific one (like “acute pain in the right knee”), the insurance company’s automated system might decide that the procedure you performed wasn’t actually necessary. Specificity in your clinical notes allows coders to use the most detailed codes, which is the fastest way to get a claim approved.
3. What are “upcoding” and “downcoding,” and why are they dangerous?
Upcoding is billing for a more expensive service than what was actually provided (like billing a complex 45-minute visit for a 5-minute check-up). This is considered fraud and can lead to heavy fines. Downcoding is the opposite—billing for a cheaper service than what was provided, often out of fear of an audit. While it’s not illegal, downcoding is a “revenue leak” that causes your practice to lose money you legally earned.
4. How does medical coding directly affect my practice’s cash flow?
Medical coding is the bridge between your work and your bank account. If a code is missing a “modifier” or doesn’t match the diagnosis, the claim is rejected. Every time a claim is rejected, it adds 30 to 60 days to your reimbursement timeline. Accurate coding ensures that about 95% of your claims are paid on the first attempt, keeping your cash flow steady.
5. Do I need to be the one actually doing the coding?
No, most providers focus on documentation, not coding. Your job is to write clear, detailed notes in the patient’s chart. A certified medical coder then reads your notes and “translates” them into the alphanumeric codes. However, you should still understand the basics so you can review denial reports and ensure your team or billing service is capturing the full value of your work.
6. What are HCPCS codes, and when are they used?
While CPT codes cover your services, HCPCS codes (pronounced “hick-picks”) are used for things that aren’t exactly medical procedures. This includes medical equipment (like crutches or a wheelchair), certain injections or drugs, and supplies. If your practice provides any physical items to patients or performs Medicare-specific screenings, you will likely see HCPCS codes on your billing statements.